British Association of Dermatologists’ guidelines for the management of bullous pemphigoid 2012
Definition
BP is an autoimmune subepidermal blistering disease that typically affects the elderly but may rarely present in children and younger adults. Autoantibodies of IgG type (and less commonly
IgA, IgM and IgE) attack components of the adhesion complex of the basement membrane zone (BMZ) and result in subepidermal blistering. The two main autoantigens are BP230 (BPAg1) and BP180 (BPAg2, collagen XVII).
Epidemiology
BP is the most common immunobullous disease in Western Europe with a reported incidence of 43 per million per year in the U.K. and 7–13 per million per year in other parts ofEurope. The mean age of onset is around 80 years. Recently it has been shown that BP is associated with neurological disease such as cerebrovascular disease, dementia, Parkinson disease, epilepsy and multiple sclerosis.
These conditions predate BP and hence are considered as risk factors.
There are a number of anecdotal case reports suggesting an association between BP and some drugs. A recent small case series reported BP occurring in five diabetic patients taking an oral hypoglycaemic agent, gliptin (dipeptidyl peptidase-IV inhibitor),together with metformin.
Two French case–control studies, both by the same author,have described a significant relationship with the use of spironolactone and neuroleptics.
A recent U.K. case–control study found an association only with furosemide after adjusting for cardiovascular and neurological disease.
The mechanism by which drugs may induce BP has not been
studied. There is no conclusive evidence for an association with malignancy or other autoimmune diseases.
Clinical presentation
Tense blisters are often seen on erythematous or normal-looking skin of limbs and trunk and may be widespread or localized. Bullae and ⁄or erosions may be present in the oral and genital
mucosa.
Pruritus alone or associated with erythema and ⁄or urticated plaques may precede formation of bullae by weeks or months; in some cases bullae may not become clinically apparent.
Laboratory diagnosis of bullous pemphigoid
A skin biopsy from a fresh blister stained with haematoxylin and eosin shows subepidermal clefting and an inflammatory
infiltrate mainly consisting of eosinophils; however, the diagnosis is confirmed with immunofluorescence studies (IF).
A biopsy for direct IF (DIF) is taken from uninvolved skin about 1 cm away from a fresh blister and is immediately snap-frozen in liquid nitrogen or transported in either Michel’s transport medium or normal (09%) saline). If using saline, the biopsy must be processed within 24–48 h; with Michel’s medium prompt handling is to be preferred, but a longer delay of up to 2 weeks may still yield results
Indirect IF (IIF) is performed on serum, and if this is not obtainable, on blister fluid.
The characteristic DIF picture in BP is a linear deposition of IgG and ⁄or C3 along the BMZ. Other immunoglobulins, including IgA, IgM and IgE, may also be present.
Substrates used for IIF include monkey oesophagus and normal human skin; the latter can be split using molar saline.
Antibodies in BP serum usually detect antigens at the roof of the salt-split skin.
In most cases this may help to differentiate BP from other immunobullous diseases such as epidermolysis bullosa
acquisita (EBA) and some cases of mucous membrane pemphigoid (MMP), in both of which antibodies are deposited
on the dermal aspect of the split skin.
Over recent years, enzyme-linked immunosorbent assay (ELISA) has emerged as an additional diagnostic technique for some autoimmune bullous diseases.
Serum levels of antibodies to both BP180 and BP230 can be measured with commercially available ELISA kits, with the BP180 ELISA being more sensitive than the BP230 ELISA.
The NC16A domain is an important pathogenic epitope of the BP180 antigen and is used in BP180 ELISA to detect antibody titres that reportedly correlate with disease activity.
In one study, false-positive ELISA results using the same commercial kits were reported in 7-4% of sera with negative IIF.
The ELISA is currently not widely available in the U.K.
but is a useful additional diagnostic tool in selected cases and in research. IF studies remain the gold standard for diagnosis.
Management
BP is usually a self-limiting disease with a clinical course that may last from months to years. During the active stage, the disease is associated with significant morbidity and a mortality twice that of the general elderly population.
Older age at onset and frail general condition are poor prognostic factors.
Many available treatments are associated with toxicity and may be poorly tolerated in patients with BP.
Mortality during the first year is significantly higher in patients treated with high doses of systemic corticosteroids (prednisolone equivalent >40 mg daily).
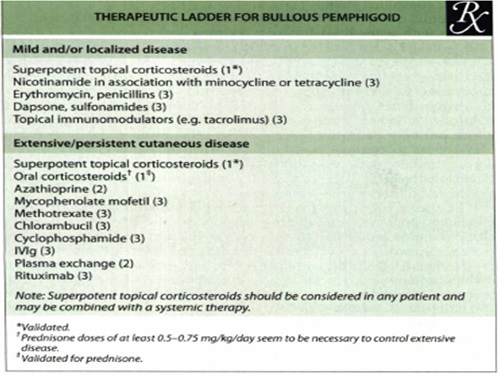
Treatment should aim to control symptoms with minimum adverse effects where possible. Options are broadly divided into anti-inflammatory drugs, immunosuppressive or immunomodulating drugs, and procedures aiming to remove circulating pathogenic antibodies and inflammatory mediators.
The choice of treatment depends on the individual patient’s circumstances especially the severity of the BP and the presence of comorbidities.
Systemic steroids (strength of recommendation A;level of evidence 1+)
Systemic corticosteroid therapy was demonstrated to be effective in BP in uncontrolled clinical studies during the1950s and has become established as the mainstay of treatment.
The effect in most cases is rapid, with suppression of inflammation and blistering typically achieved within 1–4 weeks, after which the dose is gradually reduced.
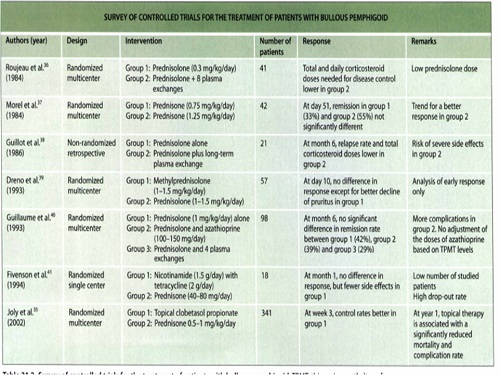
The most commonly used drugs are prednisone and prednisolone which are assumed to be bioequivalent. Serious dose dependent metabolic and immunosuppressive adverse effects were recognized in these original studies and in the four randomized controlled trials (RCTs) involving systemic steroids in the treatment of BP.
The effect of very high doses of systemic steroid was assessed in eight patients with severe widespread BP, of whom six had failed to respond to standard doses of systemic steroid.
Seven of the eight had significant medical comorbidity.
Intravenous methylprednisolone, either 1 g daily (two patients), or 15 mg kg)1 daily (six patients) for 3 days, was followed by prednisone 30–40 mg daily. All patients responded rapidly to the intravenous methylprednisolone, but in spite of the oral prednisone, blistering (albeit less severely than initially) recurred within 2 weeks.
One patient died within 1 week of the intravenous methylprednisolone, and three died between 1 and 4.5 months following the treatment.
The causes of death were cardiac arrest, infection and congestive cardiac failure.
General conclusions from the studies are:
1 .Systemic steroids are the best established treatment for BP;
2. Immunosuppressive and metabolic adverse effects occur and are dose-dependent;
3. Doses of prednisolone of (0.75-1 mg kg) daily in widespread BP are effective within 1–4 weeks in about 60–90% of cases.
Clinical experience suggests that the more severe the disease, the larger the dose of steroid is required (up to 1 mg
Kg/ daily), although this has not been rigorously proven.
A minority of patients with BP respond poorly to such doses of systemic steroid; increasing the dose confers little additional benefit and is significantly more toxic.
It is not possible to identify a starting dose of prednisolone (or prednisone) that would be maximally effective and minimally toxic for all patients with BP.
Doses which might meet these criteria for a majority of patients are:
1.(0.75-1mg kg) for patients with severe involvement;
2.(0.5mg kg) for moderate disease;
3.(0.3mg kg) for mild or localized disease.
If new inflammatory or blistered lesions are few or absent within 4 weeks, the treatment can be regarded as successful and the dose of steroid should then be gradually reduced.
A reduction of the daily dose of prednisolone at fortnightly intervals, initially by about one-third or one-quarter down to 15 mg daily, then by 2.5mg decrements down to 10 mg daily, is suggested.
The dose could then be reduced by 1 mg each month. In about 50% of cases relapse will occur at some point during the dose-reduction period, indicating that the previous dose is likely to be the minimal effective dose for that patient.
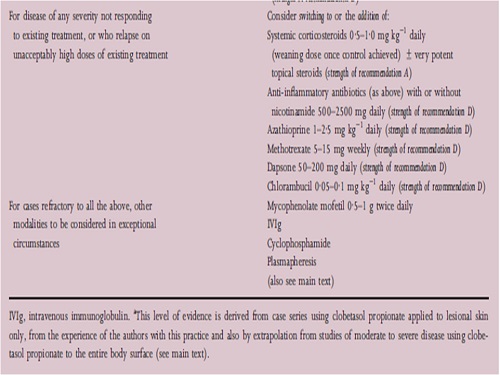
For patients with widespread BP who do not respond to these doses, or who relapse on unacceptably high doses, other agents, alone or in addition to the systemic steroid, may be preferable to higher doses of steroid.
The duration of systemic steroid treatment in BP is likely to be many months and is sometimes indefinite.
Gastric protection, usually with a proton pump inhibitor, should be considered.
Measures aimed at minimizing loss of bone density are appropriate in postmenopausal women and men over 50 years, and in any patient at increased risk of fragility fracture, who are expected to take prednisolone 7.5mg or more daily for at least 3 months.
Patients with BP (and also patients with pemphigus vulgaris) were reported to have lower levels of vitamin D, and a higher incidence of severe hypovitaminosis D, than controls, suggesting additional risk of bone density loss.
Calcium and vitamin D supplementation and a bisphosphonate are usually recommended and have been shown to be effective in preserving bone density, if given from the start of systemic steroid therapy in patients with immunobullous diseases.
Calcium may impair absorption of mycophenolate mofetil (MMF) and oral bisphosphonates and should be taken at a different time.
Topical corticosteroids (strength of recommendationA; level of evidence 1 +)
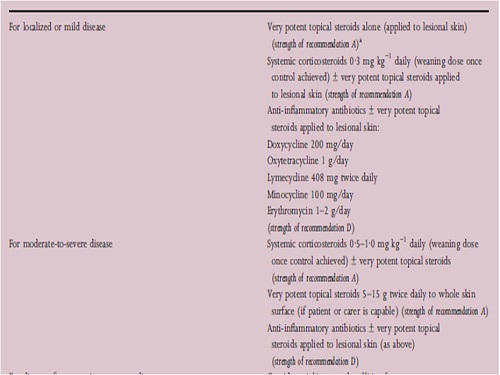
Uncontrolled studies have suggested the successful use of topical steroids as first-line treatment for both localized and moderate disease,and two recent RCTs with a total of 653 participants confirmed this view.
Topical clobetasol propionate 0.05% cream (20 g) applied all over twice daily, including clinically unaffected skin (total daily dose 40 g), was compared with oral prednisone (1 mg kg)1 daily) in the treatment of BP.
A significant benefit of the former was shown in extensive disease (more than 10 new blisters a day) for disease control, adverse events and mortality.
In the moderate-disease group (fewer than 10 new blisters a day) no significant differences were found between clobetasol propionate cream and prednisone (0.5mg kg) daily for disease control, adverse events and mortality.
Morbidity and mortality attributable to corticosteroid treatment were seen in all groups but were significantly higher in the prednisone (1 mg kg) group.
In 2009 the same group compared clobetasol propionate cream 20 g twice a day (standard regimen) with 10–30 g per day depending on disease severity and body weight (mild regimen).
Regression or healing of skin lesions at 3 weeks was achieved by nearly all patients in both regimens.
The median cumulative doses of steroid cream used during the study period were 5760 g in the standard regimen vs. 1314 g in the mild regimen, which is a 70% reduction in cumulative doses.
There was no difference regarding the relapses between the mild and standard regimens, indicating no significant difference in effectiveness between them.
The main severe side-effects in both groups were diabetes mellitus (n = 34 standard, n = 18 mild), cardiovascular and neurovascular disorders (n = 35 standard, n = 21 mild), and severe infections (n = 32 standard, n = 27 mild). There were also cutaneous sideeffects, which included purpura, severe skin atrophy and striae.
There was no significant difference between the two groups in terms of year 1 mortality rate.
In the standard regimen, mortality was 38% (58 ⁄153) [moderate disease 32% (21 ⁄65), severe disease 42% (37 ⁄88)] and in the mild regimen it was also 38% (58 ⁄153) [moderate disease 28% (19 ⁄69), severe disease 46% (41 ⁄90)].
However, the report of the study gives an adjusted analysis (Cox model adjusted for age and Karnofsky score), after which a beneficial effect of the mild regimen was observed in participants with moderate BP, with an almost twofold decrease in the risk of death or life-threatening adverse events relative to the standard regimen.
A recent survey of 1135 dermatologists in the U.K. (326 responses, 28.7% showed that 98% of respondents use topical steroids as sole treatment in localized BP and 34% in generalized BP.
It is routinely used as an adjunct (92%), mostly applied to the lesions only (86%). A total of 34% of respondents use topical steroids until remission is achieved while 66% continue to use it to deal with relapses.
Very potent topical steroids (clobetasol propionate) are an effective treatment for BP and they seem to have less serious adverse effects compared with( 1 mg kg) of prednisone per day.
However, their use in extensive disease may be limited by practical factors (e.g. ability of patient or availability of carer to apply the treatment) and they may be associated with systemic absorption and adverse events.
When feasible they should be considered for first-line treatment, especially in localized disease.
Azathioprine (strength of recommendation D; level of evidence 4)
After systemic steroids, azathioprine is still a commonly used drug in BP. It is mostly employed in doses of up to (0.5-2mg kg) daily as an adjunct to systemic steroids for its presumptive steroid-sparing effect. However, the efficacy of azathioprine as an adjunct to prednisolone in BP has been addressed in only two RCTs and with conflicting results.
One small, nonblinded RCT reported a 45% reduction in cumulative prednisolone dosage over a 3-year period.
Conversely, a larger RCT lasting only 6 months found no difference in remission rates in patients treated with steroids alone compared with those receiving combination treatment with prednisolone and azathioprine.
In fact, more adverse effects were reported in patients receiving azathioprine.
A more recent nonblinded RCT with 73 patients compared azathioprine (2mg kg) daily) with MMF 1 g twice daily as adjuncts to methylprednisolone (0.5mg kg) daily.
Remission was achieved in 100% of patients in both groups but this trial included no steroid-only arm, so no conclusions can be drawn as to the superiority of adjunctive treatment over steroids alone.
The azathioprine arm was slightly faster to produce remission than MMF (median 28.6days compared with 42 days). Both treatments were similarly effective at preventing relapses and had similar numbers of adverse events.
Hepatotoxicity was documented in six out of 37 patients treated with azathioprine but more infections occurred with MMF.
Although the treatments were equally effective, the 5.5fold higher cost of MMF (2 g daily) compared with azathioprine (2 mg kg) daily for a 75-kg patient) could be an important consideration in some health economies.
Azathioprine dose can be optimized with regard to myelosuppression risk by prior assay of thiopurine methyltransferase (TPMT) activity, a test that is now widely available in the U.K. and relatively inexpensive.
However, a normal TPMT level does not totally preclude myelotoxicity and regular monitoring of blood counts and liver function are essential.
There is currently insufficient evidence of benefit to recommend routine addition of azathioprine to systemic steroids for
the control of BP. In view of its side-effect profile, it is recommended that azathioprine only be considered as an adjunctive treatment to prednisolone where response has been inadequate and the disease is not suppressed, or where the side-effects of existing therapy are troublesome and unacceptable.
Anti-inflammatory antibiotics and nicotinamide (strength of recommendation D;)
Antibiotics with anti-inflammatoryeffects are used widely in the treatment of BP.
A German survey reported that about 10% of the dermatologists use a combination of antibiotics and nicotinamide as a first-line treatment for BP;
a survey in the U.K. showed that 80% of respondents use antibiotics as part of their management of BP.
Mostly doxycycline is used in the U.K. (40%), followed by minocycline (31%) and lymecycline (19%).
A (alltotal of 63% of respondents thought that antibiotics are sometimes effective, while 28% thought that they are never effective.
The most reported side-effect was gastrointestinal upset, followed by pigmentation and Candida infection; hypersensitivity syndrome with hypereosinophilia was only mentioned in two responses.
There are one small RCT, small uncontrolled trials and case reports on antibiotics and nicotinamide (niacinamide).
The small RCT compared six patients who received prednisone (40–80 mg daily) with 14 patients who received tetracycline 2 g per day and nicotinamide 1500 mg daily.
After 8 weeks of treatment there were one complete and five partial responders in the steroid group, compared with five complete responders, five partial responders, one non responder and one disease progression in the tetracycline group.
Two participants in the tetracycline group were unavailable for follow-up at 8 weeks; the results were not statistically significant.
Of the participants available for long-term follow-up, all five in the tetracycline group remained disease free (mean 17.5weeks) while two of the three in the steroid group had repeated flares with tapered-off treatment (mean 21.3weeks).
The side-effect profile was in favour of tetracycline and nicotinamide. There are several additional case reports and small series that describe the beneficial effect of tetracyclines, usually in combination with nicotinamide. It was helpful in the majority within 1–3 weeks; however, some patients received topical or even systemic corticosteroids in addition.
There are only two case series involving 11 and 15 patients, and many case reports, of the beneficial effect of erythromycin in children and adults. Erythromycin should be considered for treatment, particularly in children (adult dose 1000–3000 mg daily), and perhaps in combination with topical corticosteroids.
A beneficial effect may be seen within 1–3 weeks of commencing treatment.
In conclusion, tetracyclines and nicotinamide may be considered as treatment in adults, perhaps in combination with topical corticosteroids. However, apart from one case report of niacinamide (nicotinamide) as monotherapy in localized BP, there is no evidence for its effectiveness as a sole treatment of BP.
The optimum doses, both for the antibiotics and nicotinamide, are not established. Nicotinamide is used between 500 and 2500 mg daily, usually started at 500 mg daily and then gradually increased to 1500–2500 mg daily to minimize gastric sideeffects.
Tetracycline has been used at doses of 500–2000 mg daily, doxycycline at 200–300 mg daily and minocycline at 100– 200 mg daily.
Tetracycline should be avoided in renal impairment as should doxycycline and minocycline in patients with hepatic impairment. Minocycline has a worse side-effect profile and is therefore not the first choice of antibiotic.
A few cases of minocycline-associated pneumonia and eosinophilia have been described, necessitating immediate withdrawal.
Lymecycline has a beneficial side-effect profile and has been successfully used by some dermatologists (408 mg twice daily) in the U.K. without published evidence.
When blister formation is suppressed sufficiently the antibiotics and nicotinamide must be reduced slowly, one at a time, over several months to avoid relapse.
Methotrexate (strength of recommendation D; level of evidence 4)
There are no controlled trials involving methotrexate (MTX) for the treatment of BP.
Two small prospective case series of 11 and 16 patients both reported that relatively low doses of MTX (max. 15 mg weekly) can be effective at controlling BP, either as a monotherapy or in combination with topical steroids.
This was confirmed by a recent retrospective multicentre case series of 70 patients treated with MTX alone, or in combination with topical steroids.
The largest retrospective analysis compared 138 consecutive patients: 61 patients received MTX plus concomitant topical steroids 2.5-17.5mg per week, median dose 5 mg per week);
37 patients received MTX and prednisolone plus concomitant topical
steroids until cessation of new blisters; 15 patients received prednisolone only (6–40 mg daily, median dose 12 mg daily) owing to pre-existing contraindications or adverse effects with MTX, or because of physician or patient preference;
25 patients were treated with topical betamethasone gel only.
The 2-year remission was 43% for MTX, 35% for MTX and prednisolone, 0% for prednisolone and 83% for the topical steroid group.
Remission occurred after a median treatment time of 11 (MTX), 20 (MTX and prednisolone) and 2 months (topical steroid). The median cumulative MTX dose to achieve remission was 210 mg (range 20–1350 mg).
Being retrospective, the cases were unmatched for disease severity and there appears to be a higher proportion of mild cases in the patients receiving MTX as monotherapy. MTX was discontinued in five patients because of adverse effects (gastrointestinal symptoms, anaemia, liver dysfunction and alveolitis).
The most important toxicities of MTX are myelosuppression, hepatotoxicity and pneumonitis. MTX is excreted renally, which should be considered in the elderly and may explain the low doses required for disease control.
Many investigators recommend folic acid 5 mg on the non-MTX days to reduce some adverse effects, but this is not proven.
Evidence from these case series suggests that MTX can be effective at controlling BP, either as a monotherapy or in combination with topical or systemic steroids
Mycophenolate mofetil (level of evidence 1-)
MMF is an inhibitor of purine synthesis in activated T and B cells and is a generally well-tolerated immunosuppressive agent used in the prevention of renal graft rejection since 1997.
It has been reported as effective in controlling BP in doses of 0.5-1g twice daily in a small number of individual case reports, both as an adjunct to systemic prednisolone and as a monotherapy following disease relapse.
Further evidence is needed for the role of MMF in BP.
Dapsone and sulfonamides (strength of recommendation D; level of evidence 3)
There are no RCTs with respect to the use of either dapsone or sulfonamides, either as sole treatments or as adjuncts in the management of BP. Four retrospective series covering a total of 110 patients have reported experience with dapsone 50–200 mg daily or (rare cases) with either sulfapyridine or sulfamethoxypyridazine 1–1.5daily.
These were employed either as sole treatments or in combination with topical steroids.
The response rate was around 45% in three series,but only 15% (six of 41) in the fourth.
Response seems to be slower in onset than with systemic steroids.
A single, small,uncontrolled series reported a possible steroid-sparing effect in patients in whom dapsone was added to existing treatment with prednisolone and azathioprine.
Another series of 62 patients reported a complete remission rate of 32% at 2 weeks in patients treated with dapsone (0.5-1mg kg) daily in combination with systemic methylprednisolone (0.5mg kg) daily and topical steroids.
The series was retrospective with no comparator arm so no conclusion was possible as to whether there was any steroid-sparing effect.
There are individual case reports of dapsone (either alone or with oral steroids) used successfully in childhood BP.
Glucose-6-phosphate dehydrogenase deficiency predisposes to haematological side-effects and should be excluded in predisposed races (e.g. those of African, Middle Eastern and SouthAsian origin), and all patients receiving dapsone need very frequent monitoring of blood count and liver function in the early months.
The side-effect profile of dapsone and sulfonamides is potentially hazardous in the elderly.
In this age group, these treatments should be considered only if other treatments are ineffective or contraindicated, and treatment started at low doses (50 mg daily) to be increased by 50 mg daily in 2-weekly steps to a maximum of 150–200 mg daily.
Intravenous immunoglobulins (strength of recommendation D; level of evidence 3)
Intravenous immunoglobulin (IVIg) has been widely tried as an immunomodulatory agent in various autoantibody-mediated blistering diseases. Excluding cases of MMP, experience in BP is confined to a total of fewer than 41 patients in small retrospective series and case reports.
When used as a sole treatment, some patients achieved rapid and dramatic, albeit short-lived responses, with relapse occurring within 2 weeks,necessitating either further infusion or treatment with corticosteroids or azathioprine.
IVIg has been more commonly used concomitantly with oral prednisolone and other agents.
A retrospective case series reported on 15 patients with severe, unstable steroid-dependent pemphigoid or in whom there were significant treatment side-effects, and other immunosuppressants or immunomodulatory agents had failed.
Treatment was with polyvalent immunoglobulin 2 g kg) administered in equally divided doses over 3 days and overlapping with preceding treatments.
Treatment cycles were repeated initially every 4 weeks until remission, and thereafter with intervals between cycles gradually increasing.
The IVIg permitted gradual withdrawal of prednisolone over 1–5 months in all 15 patients. The report does not make clear whether all other potentially active agents were also withdrawn.
Remission was maintained over a further 17–26.5months with a mean of 14.9 further cycles of IVIg.
IVIg is well tolerated but expensive, costing £5320 per cycle of 2 g kg) in a 70-kg patient.
IVIg should only be considered as an adjunctive treatment in patients with very severe disease where rapid control is needed, or when there is failure with or contraindication to other treatments
Chlorambucil (strength of recommendation D; level of evidence 3)
In an open study, 23 patients with BP completed treatment with initial doses of prednisolone of 40–60 mg daily and chlorambucil approximately 0.1mg kg) daily. After 2 weeks, the doses of both drugs were gradually reduced.
All patients responded and none required treatment for more than 12 months.
The maintenance dose of chlorambucil after 6 weeks was 2 mg per day in most cases. The mean total steroid requirement was 1866 mg, about 50% of that previously reported for prednisone and azathioprine (3688 mg over 3 years).
The risk of haematological toxicity, especially thrombocytopenia,was emphasized, and blood counts were initially monitored weekly. One patient discontinued chlorambucil due to marrow suppression, which recovered after discontinuation.
Haematological malignancy has been attributed to chlorambucil and the authors suggest that a cumulative dose of 1 g, or treatment duration of 1 year, should not be exceeded.
In a second study from the same centre, a retrospective comparison was made between patients with BP treated with prednisolone alone (26 patients), and those treated with prednisolone and chlorambucil (19 patients).
The dose of prednisolone was 20–60 mg daily based on disease severity and patient size, reduced according to response.
Chlorambucil was started at about 0.1 mg kg) daily (0.05 mg kg) daily in ‘very elderly’ patients or if the platelet count was <250 ・ 109 L). After 2 weeks it was reduced to 0.05mg kg) daily, and after a further 4 weeks to 2 mg daily.
The mean cumulative dose of prednisolone (2685 vs.4074 mg), and the mean duration of therapy (215 vs. 392 days), were both statistically significantly lower in the chlorambucil group.
Apart from an asymptomatic reduction in platelet count below the normal range in one patient, no adverse effects were attributed to chlorambucil.
Chlorambucil as an adjunct to systemic steroids should be considered as an alternative to other more established immunosuppressants if these have failed or are poorly tolerated or contraindicated.
Careful monitoring is required for possible haematological toxicity
Cyclophosphamide
Three cases have been reported in which cyclophosphamide appeared to have a beneficial effect in otherwise refractory BP.
In the only case series detailing the effects of cyclophosphamide in BP, 10 patients were treated with systemic steroid in doses of 1–1.9 mg kg)daily prednisone equivalent and with cyclophosphamide 100 mg daily.
Three patients, who had medical comorbidities, died; four others suffered significant adverse effects involving marrow toxicity and septicaemia.
Comparing their results with published studies, the authors did not perceive a steroid-sparing effect with the cyclophosphamide, but they had no control cases on steroid alone.
Cyclophosphamide is more toxic than other immunosuppressive drugs used for BP. It may rarely be considered for exceptionally refractory disease.
Ciclosporin
Reported experience of the use of ciclosporin in BP is limited to two reports from the same centre with overlapping cases, comprising a total of seven patients treated with high doses of 6–8 mg kg) daily.
Good responses were seen in two out of four cases treated with ciclosporin alone. Three patients who had relapsed on prednisone responded to the addition of ciclosporin, and two of these relapsed after the ciclosporin was discontinued. Elevation of serum creatinine occurred in most of the patients (details not given) but was reported to be ‘significant’ in only one.
Ciclosporin cannot be recommended in the routine treatment of BP. It may rarely have a place in refractory cases but its value is likely to be limited by renal toxicity, especially in the elderly.
Topical tacrolimus (strength of recommendation D;level of evidence 3)
Individual case reports have described a response to topical treatment with the calcineurin inhibitor, tacrolimus. It has mainly been used for localized and limited generalized disease.
Chu et al.reported two cases of generalized disease treated with multiple systemic agents including oral steroids but not topical steroids.
Application of tacrolimus ointment 0.1%,3-5 g daily, allowed reduction of oral steroids and improvement was seen within 2 weeks, although follow-up data were not reported.
In a case of mild vesicular pemphigoid, reduction of oral steroids and use of potent topical steroids led to new vesicles; these ceased with the substitution of topical steroids with tacrolimus ointment 0.1% (twice daily for 2 weeks), allowing withdrawal of the oral steroids.
In other reports, topical tacrolimus has been used as the sole agent for localized disease and also in vulval pemphigoid in a child.
The use of topical tacrolimus is limited by local irritation and its price compared with topical
steroids.
It may be useful as an alternative in localized and limited disease without the disadvantage of causing skin atrophy
Biologic agents
Rituximab (strength of recommendation D; level of evidence 3) This chimeric murine–human monoclonal antibody targets CD20, the B cellspecific cell surface antigen, following which B cells may be depleted from the circulation for 6–12 months.
Only a few reported patients including two children with BP have been treated with rituximab.
The dosing regimen in most cases was a weekly infusion (375 mg m)2) for 4 weeks, followed by repeat infusion in some cases; improvement was usually seen after 4 weeks.
All treated cases had refractory disease and all but two were treated concomitantly with other immunosuppressants.
Rituximab was used as a monotherapy in two cases with concomitant BP and chronic lymphocytic leukaemia with good initial outcome but no reported follow-up data.
In general, rituximab allowed gradual withdrawal of other immunosuppressants and led to disease remission, although serious adverse events were seen in three of eight cases.
Two patients died 6 weeks and 2 years after the treatment from nosocomial pneumonia and bacterial sepsis, respectively, and a 2-year-old boy was left with persistent hypogammaglobulinaemia following a series of infections
Antitumour necrosis factor-a agents (strength of recommendation D; level
of evidence 3) :There are no trials or large case series, and there is conflicting evidence as to whether these agents treat or induce BP. Etanercept was used successfully in the treatment of a patient with BP and psoriasis,but in another case, longterm use of etanercept for rheumatoid arthritis was thought to have induced BP.
Two other reports describe adalimumab induced BP, one with features overlapping with MMP.
Other biologic agents (strength of recommendation D; level of evidence 3)
Omalizumab, a humanized monoclonal antibody that inhibits IgE binding, was used successfully to treat one infant and one adult with refractory BP but with no reported follow-up data for the adult case.
A monoclonal antibody to interleukin2 receptor of T cells (daclizumab, anti-CD25) has been used to treat a patient with BP, and in combination with rituximab in a patient with BP and concomitant graft-versushost disease (GVHD). Additional immunosuppressive treatment was needed in the first patient, and the patient with GVHD, although cleared of blisters, died after a year with sepsis.
Daclizumab is no longer produced.
Biological drugs are expensive and may be associated with potentially serious adverse effects; until further supportive evidence is available, their role in BP remains limited
Plasmapheresis and immunoapheresis (strength of recommendation D; level of evidence 3)
One RCT showed an apparent steroid-sparing effect with plasmapheresis (plasma exchange) whereas another RCT did not.
Other small case series and anecdotal case reports have used different regimens of treatment with varying outcomes.
A child with BP and inflammatory bowel disease was treated with plasma exchange in combination with extracorporeal photochemotherapy that allowed reduction of immunosuppressive agents.
Immunoapheresis is a procedure by which immunoglobulins are removed from the circulation without the need to replace the plasma. Only a few case reports describe immunoapheresis as an adjuvant treatment for BP, allowing remission with a reduced dose of systemic steroids.
Plasmapheresis and immunoapheresis have no role in the routine treatment of BP, although in cases of refractory BP or when reduction of immunosuppressive drugs is necessary due to intolerance and adverse effects, these modalities may be used as adjuvant treatment.
Childhood bullous pemphigoid
BP is rare in childhood and infancy. It may mimic the adult disease but there may be a greater predilection for involvement of the palms and soles in infants; localized vulval involvement is well recognized in later childhood.
Childhood pemphigoid may be short-lived, remitting in weeks or months. Owing to its rarity, there are no trials covering childhood or infantile cases.
The most commonly used treatment is prednisolone 1 mg kg) daily, increasing to 2 mg kg)daily in some cases.
Other treatments with reported benefit are potent topical steroids alone, erythromycin as monotherapy or with nicotinamide, as well as sulfapyridine and dapsone, both as sole treatment, or with prednisolone.
There are a small number of case reports for the use of IVIg, MMF, and in two separate cases of severe recalcitrant disease in infancy, rituximab was effective in one and subcutaneous omalizumab in another.
Although there is no evidence to support any particular treatment strategy in childhood and infantile BP, its generally short-lived and benign nature suggests that preference should be given to low-toxicity treatments such as erythromycin and topical steroids (strength of recommendation D; level of evidence 3).
Skin care in bullous pemphigoid
There are no studies on this topic and the following recommendations are based on the personal experience of the authors.
Blisters should generally be left intact if possible as this may help prevent secondary bacterial infection. When they are particularly large or in sites where they are troublesome or interfere with function, such as the sole of the foot, blisters may be pierced with a sterile needle releasing the fluid, but leaving the blister roof in place.
If there are extensive areas of erosion and open raw areas, antiseptics such as potassium permanganate as a bath or soaks, or antiseptic-containing bath oils or Oilatum Plus may be used for a few days to dry the lesions and prevent infection.
Painful eroded or raw areas may be covered with a low-adhesion dressing such as Mepitel or Atrauman held in place with soft elasticated viscose stockinette Tubifast.
It is important to ensure that such areas of erosion are included in treatment with topical steroids (clobetasol propionate).
Follow-up
BP is frequently a chronic disease and ideally patients should be followed until they are in complete remission and off all treatment.
Patients should be monitored for drug side-effects and to ensure that symptoms are controlled to their satisfaction
without excessive doses of topical or systemic treatment.
Occasional itching or lesions (if acceptable to the patient) indicates that they are not being over treated.
Once their disease is stable, an attempt should be made to wean treatment at roughly 2–4 weekly intervals; this should be done on clinical criteria rather than by IF testing.
Summary
Both systemic and topical steroids have good evidence of efficacy and remain the most widely used first-line treatments.
Topical steroids may be used as an adjunct to any other treatment or used as a monotherapy, either locally applied to lesions (for localized disease) or all over the skin (if feasible) as an alternative to systemic steroids.
Anti-inflammatory antibiotics have a smaller evidence base for efficacy (trial data expected in 2013) but are widely used and may be a safer treatment for patients with comorbidities of diabetes or hypertension,and for children.
There is some evidence to support the use of azathioprine, MTX, dapsone and chlorambucil.