A 45 year old man admitted in thorax ward with chief complaint of dyspnea.
The intial diagnosis was tension pneumothorax and the special care was done
He was consulted for skin lesions the doubted
diagnosis was neurofibromatosis .
The lesions were pedanculated papules just like ,they were multiple and most located around his neck
Other lesions were like giant comodens they were also multiples and around his neck
Other lesions were translucent papules all over his back
He also had just one café a lait and a nevus depigmantosus on his abdomen
In past medical history he had another attack of tension pneumothorax 2 years ago
No history of smoking
And no other abnormality was found
Family history was also negative
Lab test were all normal








What is your diagnosis?
Birt-Hogg-Dubé syndrome
Birt-Hogg-Dubé syndrome (BHD) is an autosomal dominant condition characterised clinically by skin fibrofolliculomas, pulmonary cysts, spontaneous pneumothorax, and renal cancer.
The condition is caused by germline mutations in the FLCN gene, which encodes folliculin; the function of this protein is largely unknown, although FLCN has been linked to the mTOR pathway.
Patients can present with skin signs and also with pneumothorax or renal cancer.
Signs and symptoms
Birt–Hogg–Dubé syndrome affects the skin and increases the risk of certain types of tumors. The condition is characterized by multiple noncancerous tumors of the hair follicles, particularly on the face, neck, and upper chest. These growths typically first appear in a person's twenties or thirties. People with Birt–Hogg–Dubé syndrome also have an increased risk of developing cancerous or noncancerous kidney tumors (chromophobe renal cell carcinoma and oncocytoma, respectively) and possibly tumors in other organs and tissues
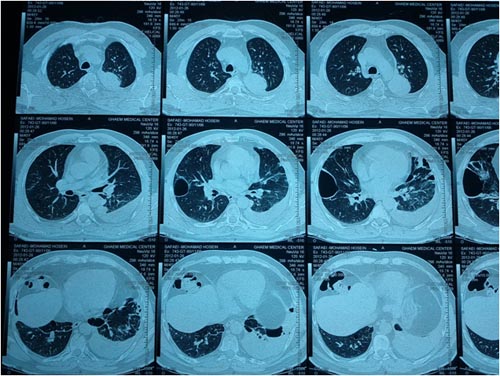
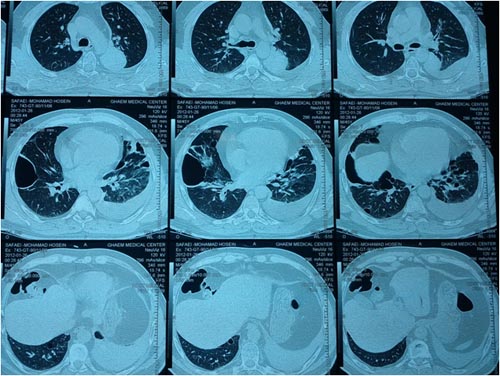
Additionally, affected individuals frequently develop cysts in the lungs that are at risk to rupture and cause an abnormal collection of air in the chest cavity (pneumothorax) that may result in the collapse of a lung.
Cause
Mutations in the FLCN gene, located on the short arm of chromosome 17 (17p11.2), cause Birt–Hogg–Dubé syndrome.
These mutations are often passed from one generation to the next in an autosomal dominant fashion but can occur as a new mutation in an individual with no prior family history.
Pathophysiology
The FLCN gene eates a protein called follicullin The normal function of this protein is still being investigated, but it appears to act as a tumor suppressor. Tumor suppressors normally prevent cells from growing and dividing too rapidly or in an uncontrolled way. Mutations in the FLCN gene may interfere with the ability of folliculin to restrain cell growth and division, leading to the formation of noncancerous and cancerous tumors. Recent studies suggest that folliculin accomplishes this function through its involvement with cellular metabolism, possibly through modulation of the mTOR pathway and/or oxidative phosphorylation in mitochondria].
People with BHD are born with one mutated copy of the FLCN gene in each cell. During their lifetime, random mutations might inactivate the normal copy of the gene in a subset of cells. When this occurs, the result is that these cells have no functional copies of the FLCN gene, allowing the cells to divide uncontrollably and form tumors. This loss of heterozygosity is a common mechanism in cancer, and it is frequently detected in the renal cancers associated with BHD ]. The molecular genetic defects in renal tumors of people with BHD are different from two other similar kidney tumors, chromophobe renal cell carcinoma and renal oncocytoma
Diagnosis
BHD can be suggested by clinical findings but is definitively diagnosed by molecular genetic testing to detect mutations in the FLCN gene. The classical clinical triad includes: 1) benign growths of the hair follicles,
2) pulmonary cysts and spontaneous pneumothorax, and
3) bilateral, multifocal renal tumors.
Clinical triad
1. The cutaneous manifestations of BHD were originally described as fibrofolliculomas (abnormal growths of a hair follicle), trichodiscomas (hamartomatous lesions with a hair follicle at the periphery, often found on the face), and acrochordons (skin tags). Cutaneous manifestations are confirmed by histology.
2. Most individuals (89%) with BHD are found to have multiple cysts in both lungs, and 24% have had one or more episodes of pneumothorax. The cysts can be detected by chest CT scan.
3. Renal tumors can manifest as multiple types of renal cell carcinoma, but certain pathological subtypes (including chromophobe, oncocytoma and oncocytic hybrid tumors) are more commonly seen in BHD.
Although the original syndrome was discovered on the basis of cutaneous findings, it is now recognized that individuals with BHD may only manifest the pulmonary and/or renal findings, without any skin lesions
Genetic testing
FLCN mutations are detected by sequencing in 88% of probands with BHD. This means that some people with the clinical diagnosis of BHD have mutations that are not detectable by current technology, or that mutations in another currently unknown gene could be responsible for a minority of BHD cases. Genetic testing can be useful to confirm the clinical diagnosis of BHD and to provide a means of determining other at-risk individuals in a family.
The prognosis depends on associated internal disease.
Papillary renal cell carcinoma has malignant potential, while pure renal oncocytomas are benign.
Evaluate colonic polyps for malignant potential.
Differential diagnosis
Trichilemmoma
Trichoepithelioma
Imaging Studies
Conduct renal ultrasonography, MRI or CT; CT scanning of the abdomen and pelvis; chest radiography.
Birt-Hogg-Dubé syndrome (BHDS) has been reported in association with various types of renal tumors, such as oncocytoma and a variant of papillary renal cell carcinoma. Birt-Hogg-Dubé syndrome is autosomal dominant; therefore, screen patients and their relatives for renal cancer. Because renal neoplasms often are asymptomatic during the growth phase, an earlier onset of fibrofolliculomas and trichodiscomas may serve as a marker.
Screening chest radiography should be advised for patients and family members because of the Birt-Hogg-Dubé syndrome association with recurrent spontaneous pneumothorax, bullous emphysema, and lung cysts. A significant association is apparent between the number and location of lung cysts and pneumothorax
Other tests
Consider colonoscopy. Colonic polyps and colonic adenocarcinoma have been previously reported as associated findings of Birt-Hogg-Dubé syndrome; however, one study in a large cohort of patients with Birt-Hogg-Dubé syndrome did not confirm a colorectal cancer association
procedure
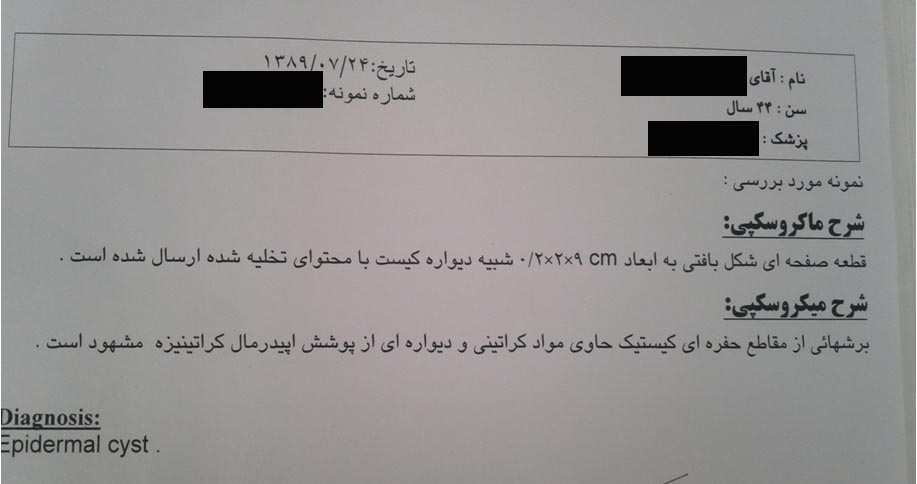
Skin biopsy is necessary to confirm trichodiscomas, fibrofolliculomas, and perifollicular fibromas.
prevention
Birt-Hogg-Dubé syndrome (BHDS) cannot be prevented, but associated findings of renal carcinoma, pulmonary cysts, and pneumothoraces can be monitored.
Advise Birt-Hogg-Dubé syndrome patients regarding the increased risk of pneumothorax with activities altering ambient pressure, such as scuba diving and air travel, particularly if they have chest pain or shortness of breath.[15]
Encourage smoking cessation in BHDS patients as smoking may be a risk factor for spontaneous pneumothorax and renal cancer.
No specific medical treatment exists for the cutaneous lesions of Birt-Hogg-Dubé syndrome (BHDS).
Surgical removal has provided definitive treatment of solitary perifollicular fibromas.
Electrodesiccation may be helpful for the removal of multiple lesions; however, lesions can recur.
Dermabrasion has been suggested as a treatment option. Lesions may recur.
Several cases of Birt-Hogg-Dubé syndrome cutaneous lesions treated successfully with carbon dioxide and Er:YAG laser skin resurfacing have been reported.
Consultations
The principle concern of Birt-Hogg-Dubé syndrome is comorbid internal neoplasms. Associated conditions most commonly include renal cell carcinoma, pulmonary cysts, and spontaneous pneumothoraces.
Refer patients with Birt-Hogg-Dubé syndrome to a family medicine or internal medicine physician for annual physical examinations and screening using renal ultrasonography and CT scanning of the abdomen and pelvis. Screening chest radiography should also be performed.
Consider referral of patients to a gastroenterologist for colonoscopy.
Refer patients to a genetic counselor, because Birt-Hogg-Dubé syndrome is a genodermatosis. Consider genetic testing to confirm the diagnosis in patients suspected of having Birt-Hogg-Dubé syndrome.
prognosis
The prognosis depends on associated internal disease.
Papillary renal cell carcinoma has malignant potential, while pure renal oncocytomas are benign.
Evaluate colonic polyps for malignant potential.
Patient education
Instruct patients with Birt-Hogg-Dubé syndrome to encourage family members to be screened using renal ultrasonography and CT scanning of the abdomen and pelvis because Birt-Hogg-Dubé syndrome is autosomal dominant.



