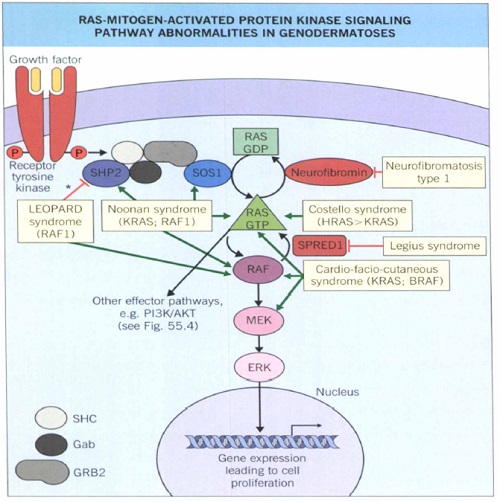
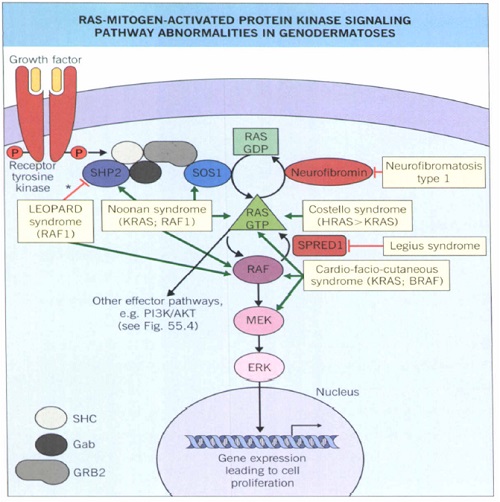
Cardiac manifestations of cutaneous disorders2012 by the American Academy of Dermatology• This review will describe primary cutaneous disorders with potential cardiac manifestations, including :• congenital syndromes, • inherited cutaneous disorders associated with later cardiovascular disease, • syndromes associated with early cardiovascular pathology.• The dermatologist may be the first to diagnose cutaneous findings associated with underlying cardiovascular disease.CONGENITAL SYNDROMES • The RASopathies• Other congenital syndromes• The Ras/MAPK pathway plays a critical role in regulating cellular function .• Each RASopathy exhibits different phenotypic features but they share certain characteristics including cardiac malformations and cutaneous abnormalities .



Noonan with multiple lentigines syndrome
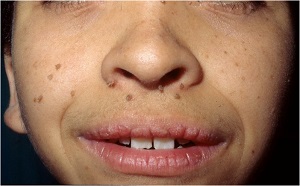
• This autosomal dominant (AD) disorder, also known as cardiocutaneous lentiginosis syndrome or multiple lentigines syndrome, has a slightly higher male predominance.
• Noonan with multiple lentigines syndrome was formerly known as LEOPARD syndrome, representing: Lentigines, Electrocardiographic (ECG) abnormalities, Ocular hypertelorism, Pulmonic stenosis, Abnormalities of genitalia, Retardation of growth, and Deafness.
The hallmark cutaneous finding is :• multiple darkbrown lentigines involving the face, neck, and upper aspect of the trunk, while sparing mucosal surfaces.
Cardiac abnormalities typically manifest as• pulmonic stenosis • hypertrophic cardiomyopathy
• Pulmonic stenosis, with a dysplastic pulmonic valve, occurs in 40% of affected individuals.
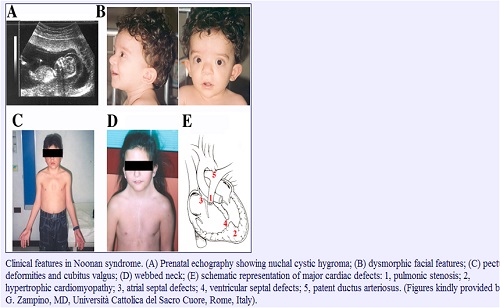
Noonan syndrome
• NS is a genetically heterogeneous AD disorder characterized by postnatal growth retardation, distinctive facial dysmorphism, cardiac defects, and variable cognitive deficits.
• patients with PTPN11 mutations generally have a higher prevalence of pulmonic stenosis, short stature, sternal deformity, and bleeding diathesis.
• patients with mutations in SOS1 present with more ectodermal abnormalities, such as keratosis pilaris and curly hair.• Other cutaneous findings include cutis verticis gyrata and lymphedema.
• Congenital heart disease occurs in 50% to 80% of individuals.Pulmonic stenosis is most frequent.
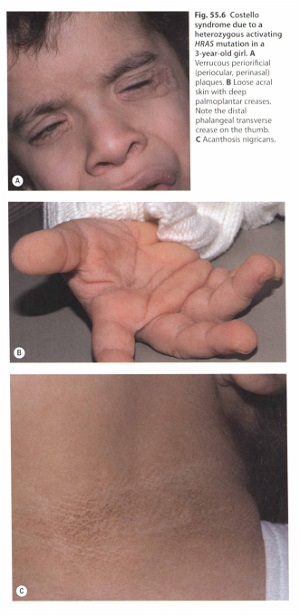
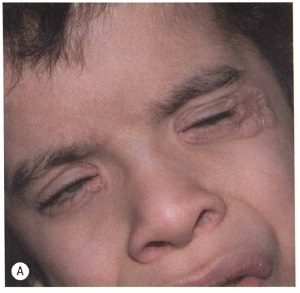
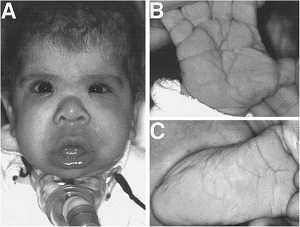
Costello syndrome.
• This AD condition is characterized by failure to thrive with severe feeding difficulties in infancy, short stature, developmental delay, and diffuse hypotonia with joint laxity.Cutaneous findings• include lax skin on the hands and feet, • Deep palmoplantar creases, • periorificial papillomas, • acanthosis• nigricans, • sparse curly hairCardiac manifestations• Most commonly pulmonic stenosis,• hypertrophic cardiomyopathy, • and arrhythmias.
• Affected individuals are at increased risk of rhabdomyosarcoma and other malignancies.
• Routine investigation for cardiac manifestations includes echocardiography; if studies at age 6 to 12 months reveal normal findings, follow-up studies are performed at the discretion of a pediatric cardiologist every 1 to 3 years until age 5 to 10 years, and then every 3 to 5 years.
Neurofibromatosis-1
• Numerous cutaneous neurofibromas and dysmorphic facial features.
• cafe au lait macules • intertriginous freckling.

Cardiac manifestations20
• heart defects, namely :
• Pulmonic stenosis, • aortic valve stenosis, • aortic coarctation.
• Four-extremity blood pressure measurement should be performed in children suspected of having coarctation, and echocardiography should be requested to evaluate a suspicious murmur.CFC syndrome
• CFC syndrome is an AD disorder caused by a number of mutations in the Ras/ MAPK pathway.
• Although many features are shared with NS, individuals with CFC syndrome have a higher frequency of ectodermal abnormalities and mental retardationCutaneous findings• generalized ichthyosis-like scaling; • keratosis pilaris; • sparse curly, • friable hair• absent eyebrows and eyelashes;• ulerythema ophryogenes; • eczema; • palmoplantar hyperkeratosis.
• Numerous acquired melanocytic nevi was the most striking dermatologic finding in 1 report
• The lack of multiple cafe au lait macules may be a distinguishing feature from NS and NF-1.
Cardiac defects• pulmonic stenosis • other valvular dysplasias, • atrial septal defects, • Hypertrophic cardiomyopathy, • patent ductus arteriosus,• rhythm disturbances, • Tetralogy of Fallot
 |
 |
Other congenital syndromes associatedwith cardiocutaneous pathology.
Carney complex
• Carney complex, previously reported as:
• NAME (Nevi, Atrial myxoma, Myxoid neurofibromas, and Ephelides)
• LAMB (Lentigines, Atrial myxoma, Mucocutaneous myxoma, and Blue nevi)
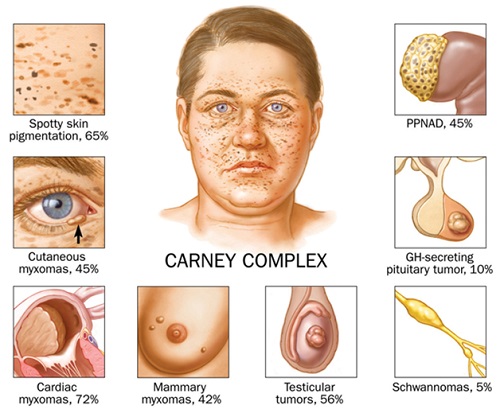
• It accounts for 7% of all cardiac myxomas.
• Lentigines are often the first manifestation and involve particularly the face, vermillion border of the lips, conjunctiva, sclera, and oral mucosa.
• Although similar to those seen in Noonan with multiple lentigines syndrome, the presence of mucosal involvement is a distinguishing factor in Carney complex.
• Annual echocardiographic surveillance for cardiac myxomas should begin at age 5 years in individuals given the diagnosis of Carney complex.
H syndrome
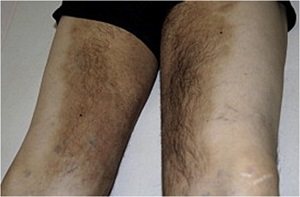
• H syndrome is an autosomal recessive (AR) genodermatosis characterized by progressive sclerodermoid skin changes with overlying hyperpigmentation and hypertrichosis.
• the thighs is most commonly affected, with variable involvement of the genitalia, lower aspect of the trunk, and limbs, and typical sparing of the knees and buttocks.
• Onset is usually between ages 1 and 20 years.
Other findings
• Hepatosplenomegaly, • Heart abnormalities,• Hypogonadism, • Hyperglycemia/diabetes mellitus,• Hallux valgus, • and decreased Height.
Cardiac abnormalities
• aAtrial or ventricular septal defect, • mitral valve prolapse, • and cardiomegaly.
INHERITED CUTANEOUS DISORDERS
ASSOCIATED WITH CARDIOVASCULARDISEASE
• Matrix protein mutations
• Inborn errors of metabolism.
Pseudoxanthoma elasticum
• This AR connective tissue disorder is caused by mutations in the ABCC6 gene on chromosome 16.
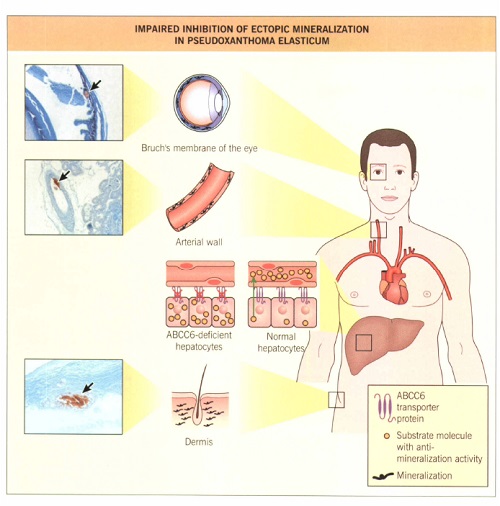
• yellow waxy papules in intertriginous and flexural areas including the neck, antecubital and popliteal fossae, and inner lower lip,
• With sparing of the scalp, palms, and soles.
• lax skin resembles ‘‘plucked chicken skin.’’

• Cardiovascular findings include mitral valve prolapse and restrictive cardiomyopathy,
• but premature atherosclerotic vascular disease is the most serious complication.
• Myocardial infarction, • renovascular hypertension,• cerebral ischemia, • intermittent claudication
• Sudden death can occur as early as age 4 years.
• Histopathologic findings include:
• Fragmentation and calcification of elastin fibers in the mid dermis, and mineralization of small and medium arteries.
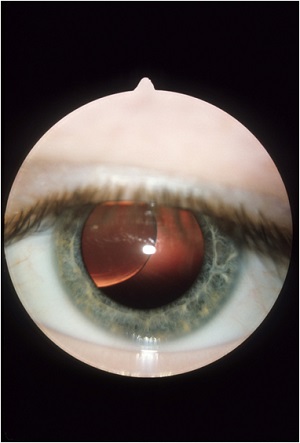
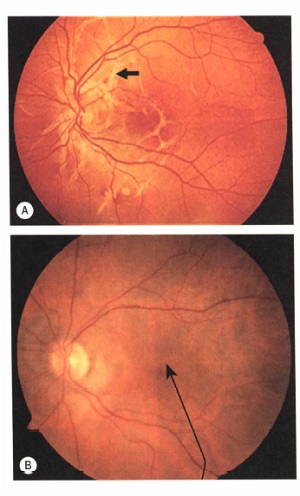
• Ocular findings are another hallmark of the disease.
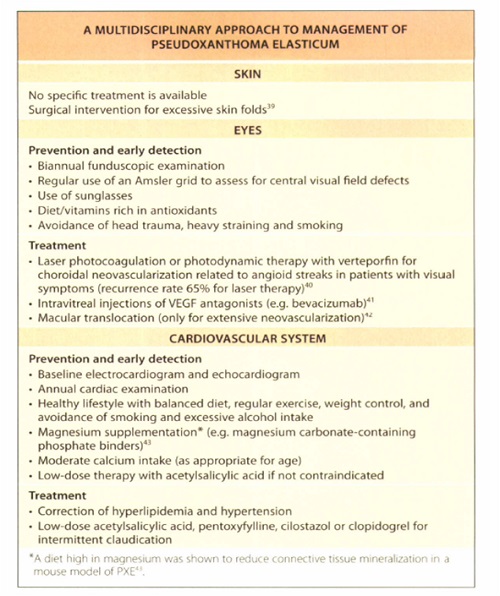
• There is no effective treatment for PXE.
• oral phosphate binders, such as sevelamer
• Cardiovascular risk factors
• dietary calcium intake
• First-degree relatives
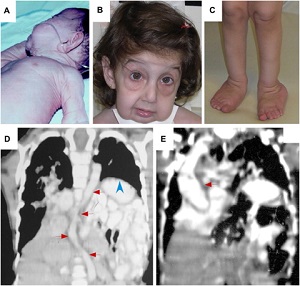
• Several bizarre appearances of the neonate were noted, including:• arachnodactyly,cyanosis, generalized pale appearance, rigidity and contracture of bilateral elbows, knees, and shoulder joints.
• Also, Gr. II/VI systolic murmur over left lower sternal border was found during acoustic examination.
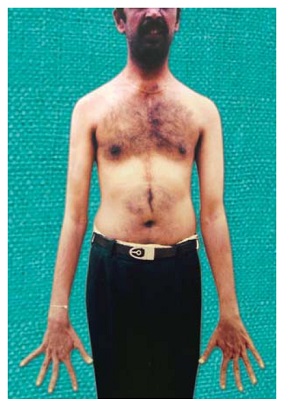
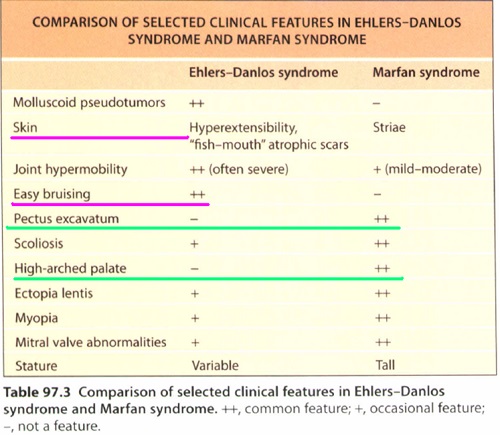
Marfan syndrome
• This AD disorder of variable penetrance is typically caused by a mutation in the gene encoding fibrillin-1, located on chromosome 15q.
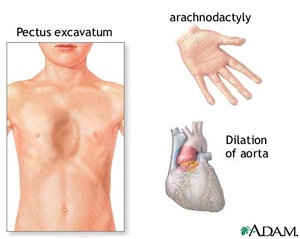
• Cutaneous manifestations include :
• extensive striae over the trunk,breasts,…• Elastosis Perforans Serpiginosa;• decreased subcutaneous fat.
• Cardiovascular changes include :
• dilation and dissection of the ascending aorta• The aortic valve regurgitation• mitral valve prolapse and regurgitation.
• All patients should undergo slit-lamp eye examination and an echocardiogram;
• annual echocardiographic surveillance and maintenance of a normotensive state with b-adrenergic blocking agents are essential.
• A 13-year-old boy was referred to our department because of easy bruising. He was born prematurely at 35 weeks and 6 days via spontaneous vaginal delivery to non-consanguineous healthy parents. Except for hypotonia at birth, the remaining perinatal and antenatal history was unremarkable. His younger brother was asymptomatic and there was no family history of premature sudden death or relevant diseases•
• He had a history of bruising and hematomas after trivial injuries and bilateral inguinal hernia repair at the age of 9.
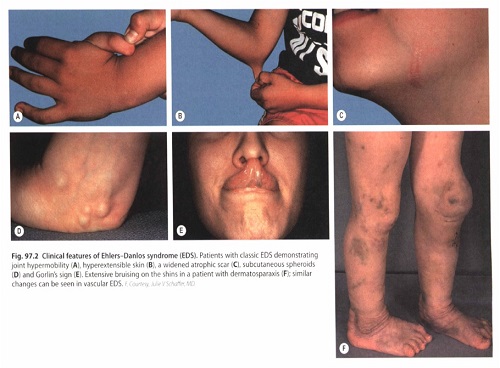
• Physical examination revealed a thin, smooth, soft, translucent and slightly extensible skin, with highly visible subcutaneous vessels. An elongated face with pinched nose, thin upper lip, high-arched palate, small chin, prominent bulging eyes, and long eyelashes was also evident. In addition, hyperpigmented, speckled, prematurely aged skin of the extremities was noted. Other associated abnormalities were hypermobility, particularly of the small joints, dorsal kyphosis, genu valgum, flat feet, long upper limbs, low muscle tone, and multiple ecchymoses, especially on the legs.Figure 1. Clinical appearance of our patient. Note the translucent skin with visible underlying vasculature, slightly extensible skin, acrogeria, small joint hypermobility, characteristic facies, ecchymosis on the legs, genu valgum, elongated upper extremities, and dorsal kyphosis.

Ehlers-Danlos syndrome.
• Individuals affected with the classic type (types I and II) may present with ‘‘cigarette paper’’ scars, and ‘‘fish mouth’’ appearance of scars, typically over the elbows and knees.
• The hypermobility type (type III) is characterized by generalized joint hypermobility.
• individuals affected with the vascular type (type IV) have thin, translucent skin and diffuse ecchymoses. • Elastosis perforans serpiginosa may be observed in the vascular type.
• Cardiac findings :
• aortic root dilation, • mitral and tricuspid regurgitation or prolapse in the classic and hypermobility types.
• arterial aneurysms, • dissection, • Rupture in vascular type.
• a recent randomized trial of celiprolol, a long-acting b1 antagonist with partial b2-agonist properties, has shown promise in decreasing the incidence of arterial rupture or dissection in patients with vascular Ehlers-Danlos syndrome.
• A 9-month-old female patient presented with cough and breathlessness of 1 week's duration. • She was found to have loose, sagging skin all over the body since birth. • Her developmental milestones were normal and she had no past history of major illness.. • At the time of presentation she had moderate respiratory distress with a respiratory rate of 38/min, a pulse rate of 132/min, and temperature of 100°F. On examination, apart from right upper zone crapitations, a diastolic murmur was heard.
cutis laxa
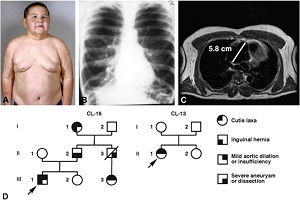
• Elastolysis or dermatochalasia, cutis laxa is characterized by progressive generalized loss of skin elasticity with skin looseness.
• Cutis laxa may be acquired or inherited as an AD, AR, or X-linked disorder.
• There are 3 distinct types of cutis laxa, with cardiac involvement in types I and III.
• Cardiac findings include aortic dilation and rupture, peripheral pulmonic stenosis, and right heart failure.
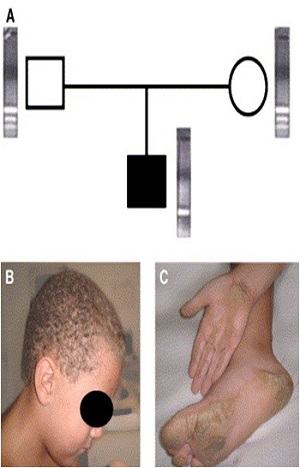
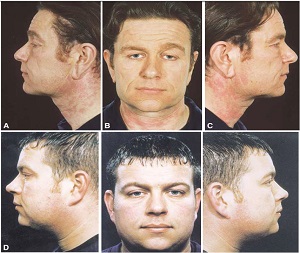
• Pulmonary emphysema may manifest in childhood, with resultant right-sided heart failure.. Manifestations and inheritance of autosomal dominant (AD) cutis laxa (CL). A, Photograph of patient at age 13 years. B, Chest X-ray of 51-year-old patient with severe emphysema shown by bilateral hyperexpanded lung fields (reprinted with permission16). C, Magnetic resonance imaging of aortic root in patient indicates aneurysm of 5.8 cm (white bar).
Manifestations of autosomal recessive cutis laxa type II. A, Redundant and wrinkled skin in patient. B, Craniofacial features include short nose, broad nasal bridge, down-slanting palpebral fissures, bitemporal narrowing, broad forehead, and retrognathia. C, Brain magnetic resonance imaging showing thickening of gray matter and pachygyria
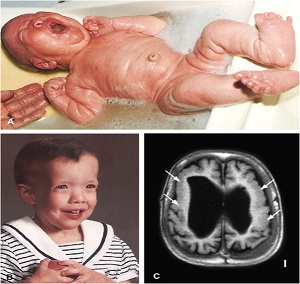
Fig 4. Manifestations of autosomal recessive cutis laxa type I. A, Redundant skin and large ears in patient with fibulin-5 mutation (reprinted with permission23). B, Sagging cheeks and periorbital area, reverse-V eyebrows, long philtrum, and large ears in patient with fibulin-4 mutation. C, Redundant skin and joint laxity on the legs of a patient with ARCL-I (reprinted with permission31). Computed tomography images of tortuous aorta (arrows) and diaphragmatic hernia (arrowhead) in patient with fibulin-4 mutation (D) and aortic aneurysm (arrow) in patient with fibulin-4 mutation (E).
• Matrix protein mutations
• Inborn errors of metabolism.
• A six year-old boy was admitted to the hospital with vision problems.• Ophthalmologic examination revealed a lens dislocation . • The child had a marfanoid stature.Homocystinuria.
• This AR disorder is caused by homozygous cystathionine b-synthase deficiency, which results in accumulation of homocysteine and disruption of normal collagen cross-linking.
• Cutaneous findings include :• livedo reticularis, • Malar rash, • ‘‘tissue paper’’ scars, • large facial pores, • Sparse fine hair, • dyspigmentation, • and superficial thrombophlebitis.

• Elevated plasma homocysteine levels lead to : increased platelet adhesiveness with resultant atherosclerosis, arterial and venous thrombosis, and pulmonary embolism.
• An independent risk factor for atherosclerosis;
• One third of patients will have a thrombotic event typically before age 30 years.
Treatment of homocystinuria:
• vitamin B6 (pyridoxine) therapy,• protein-restricted and methionine-restricted diets,• oral betaine• folate and vitamin B12 supplementation.
• Oral contraceptives should be avoided because of the additive risk of thrombotic events.
• prophylactic anticoagulation is recommended in the third trimester of pregnancy and postpartum period.
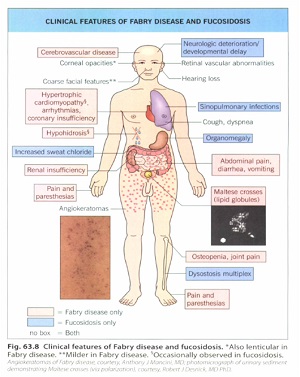
Fabry disease
• this X-linked recessive disorder is caused by a-galactosidase A deficiency, which results in accumulation of a trihexoside within lysosomes.
• Affected patients commonly experience episodes of severe pain in the extremities.
• The hallmark cutaneous finding is angiokeratoma corporis diffusum universale.
• punctate telangiectasias in the axillae and on the upper aspect of the chest.• hypohidrosis or anhidrosis .
• hypertrophic cardiomyopathy, • Valvular abnormalities, • conduction defects, • hypertension,• progressive atherosclerotic disease
• Cardiovascular disease and renal failure are the primary causes of death in patients with Fabry disease.
• Diagnosis is based on the clinical findings and confirmed by decreased levels of a galactosidase A in plasma and fibroblasts.
• Enzyme replacement therapy has been used as a successful treatment for Fabry disease since 2001.
• This treatment improves cardiac structure and function, with optimal outcome when therapy is instituted early in the disease course.

• A recent prospective cohort study found that xanthelasmata are a cutaneous marker of atherosclerosis independent of serum lipid levels and should therefore be considered a risk factor for myocardial infarction, and ischemic heart disease.SYNDROMES ASSOCIATED WITH EARLY CARDIOVASCULAR PATHOLOGY

Progeria
• Hutchinson-Gilford progeria syndrome is an AD premature aging syndrome characterized by features of normal aging such as skin wrinkling, alopecia, and osteoporosis.
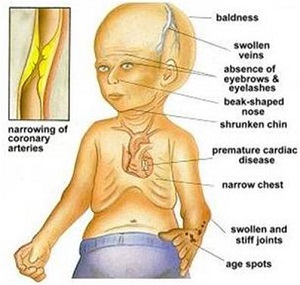
• Patients have premature and accelerated atherosclerosis, which results in heart attack or stroke at a mean age of 13 years.
• Cardiovascular pathology is characterized by loss of smooth muscle cells in the medial layer of the descending aorta, other large and small arteries, and arterioles, along with intimal thickening and calcification.
• Importantly, inflammation and lipid deposition in the intima, as observed in atherosclerotic plaques, is not observed.
• Concentric left ventricular hypertrophy is often present, even in the absence of elevated blood pressure.
• Dyslipidemia is not a defining feature, although children with Hutchinson-Gilford progeria syndrome have decreased high-density lipoprotein levels.
Werner syndrome
• Often referred to as ‘‘adult progeria,’’ this AR disorder is characterized by premature graying, alopecia, sclerodermoid changes, loss of subcutaneous fat, ankle ulcerations, and premature atherosclerosis.
• Cardiovascular disease is typically valvular, with frequent calcification, mitral regurgitation, or aortic stenosis.

PHACE syndrome
• PHACES, representing: • Posterior fossa malformations,• Hemangiomas, • Arterial anomalies, • Cardiacdefects and Coarctation of the aorta, • Eye anomalies,• Sternal defects and Supraumbilical raphe.

• Reported cardiovascular abnormalities are divided into major and minor criteria.• Major cardiovascular features include:
• aortic arch anomalies, such as aortic coarctation, aneurysm, • aberrant origin of the subclavian artery with or without a vascular ring.
• Minor cardiovascular abnormalities include:• Ventricular Septal Defects and • a double aortic arch.
• Aortic coarctation is the most frequently described cardiovascular abnormality.
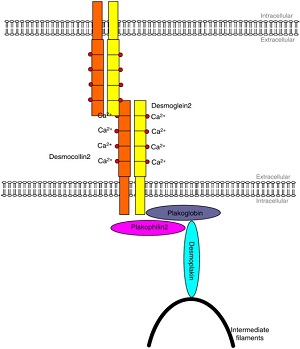
Naxos disease
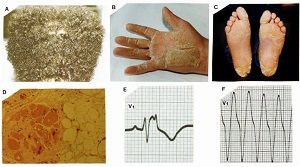
• Initial manifestations of Naxos disease include diffuse nonepidermolytic palmoplantar keratoderma and woolly scalp hair, which may be hypopigmented and present at birth.
• The hallmark cardiac finding is arrhythmogenic right ventricular cardiomyopathy, which typically becomes symptomatic in adolescence with syncope and arrhythmias.
• ECG abnormalities are present in nearly 100% of adults. Sudden death from arrhythmia is a major cause of death and typically affects patients in the fourth decade of life.
Carvajal syndrome
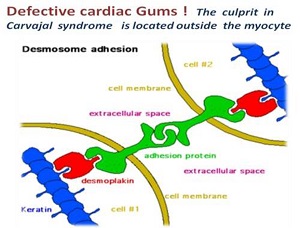
• Cutaneous findings include striate epidermolytic palmoplantar keratoderma, woolly scalp hair, skin fragility, and fingernail clubbing. Patients may experience transient pruritic blistering on the trunk or extremities, resulting fromacantholysis of the spinous epidermal layers.

• In contrast to Naxos disease, cardiac involvement is characterized by a primarily left-sided dilated cardiomyopathy.
• There does appear to be some overlap between the cardiac findings in Naxos disease and Carvajal syndrome, and the outcomes may result from a similar desmosomal defect.


It is important for the dermatologist to be cognizant of disorders with cardiac involvement, so that timely referral for evaluation and management may be undertaken.